
CALD suicide deaths – who counts?

In late November 2025, the ABS issued released its generalised causes of death data report for 2024.
This data received significant media attention, largely as it heralded to rise of dementia as the leading cause of death (9.4%) surpassing ischaemic heart disease (8.7%) for the first time. Without diminishing the enormity of this result, as a member of the National Office of Suicide Prevention’s Advisory Board, I was particularly interested in the data relating to suicide - which reported a headline figure of 3,307 lives lost in 2024.
This figure warrants close attention, as its makeup reveals a detailed and complex picture. The following key pieces of information have been taken from a detailed summary of the data developed by Suicide Prevention Australia.
The median age of death by suicide was 46 years, compared to 82for all causes of death.
Suicide was the 16th leading cause of death overall, remaining unchanged from 2023.
Suicide accounted for 15.9% of all child deaths in 2024.
Males have continued to account for over three quarters (76.5%) of deaths by suicide with males aged 60-64 having the largest increase in age-specific suicide rates from 2023-24 (an 18% increase).
Females aged between 25-29 years had the highest age-specific suicide rate of females aged under 85 years (9.8 deaths per 100,000), with the highest proportion of suicide occurring in those aged between 25-29 years (12.3%).
Suicide was the 5th leading cause of death for Aboriginal and Torres Strait Islander people. For men it was the 2nd leading cause and 10th for females in 2024.
Over the five-year period 2020-2024, suicide was the leading and second leading cause of death for female and male Aboriginal and Torres Strait Islander children, respectively.
There is far less clarity around suicide in Australia’s culturally and linguistically diverse (CALD) communities. If you can’t count it, you can’t see it, so nothing needs to be done about it.
This is a problem in both equity terms and in the effective pursuit of suicide prevention.
The data on death by suicide includes a limited measure of ethnicity - country of birth (COB). However, as the Australian Bureau of Statistics states in its explanatory notes, “deaths without a recorded country of birth are excluded”. From a demographic analysis perspective, COB falls far short of the minimum data set required to meaningfully analyse suicide incidents by ethnicity. It also prevents access to more granular level of data to assist in understanding relevant demographic and behaviour demographic and behavioural information that could help identify relevant intersections and guide targeted action in CALD suicide prevention.
Without other ethnicity data we cannot meaningfully explore potential cultural differences for people from CALD backgrounds born in Australia nor can we consider the impact of length of residence on suicide.
There is some debate about what should be captured in a minimum data set, but as a practitioner and advocate for many decades, I believe the following elements are essential for understanding suicide:
Country of birth captures a person's country of origin.
Main languages spoken at home identifies the primary language spoken in a person's household, other than English.
Proficiency in spoken English measures a person's English-speaking ability.
Year of arrival in Australia includes the year a person arrived in the country.
The year of arrival data often sits outside the first three in a minimum set, but I have included it as an important factor given the data and insights presented and discussed below.
Aggregation issues and insights
County of birth data is treated in two ways in the ABS’ Report.
The first is by Standard Australian Classification of Countries (SACC). This approach aggregates countries of birth into broader regions such as:
Oceania and Antarctica
North-West Europe other than UK and Ireland
Southern and Eastern Europe
North Africa and the Middle East
South-East Asia
North-East Asia
Southern and Central Asia
Americas
Sub-Saharan Africa
The data shows that over the five-year period 2020 to 2024, those born in Australia had a higher age-standardised suicide rate compared to those born in other regions. The suicide rate for people born in Australia was 14.6 per 100,000 - 1.8 times higher than the rate for those born overseas (8.3 per 100,000). The largest difference was between those born in Southern and Central Asia where the suicide rate was close to 3.5 times lower than those born in Australia.
An initial consideration of this data might suggest that migration, and the subsequent settlement of migrants into Australia, could highlight the protective and cultural factors that mitigate against suicide and suicidality - factors such family support, cultural and religious taboos associated with suicide and familial obligations. This is a pure assumption as there is limited research focused on this phenomenon, but one that is worth looking at if we are trying to develop effective suicide prevention strategies across the Australian community.
The other significant information in the data set is the median age of suicide deaths in this overseas born cohort. While the Australian born median age for suicide deaths is 34.5 years, the overseas born figure is 43.9 years which for those from Southern and Eastern Europe with the mean age for southern Europe being 71.4 years and South-Eastern Europe 66.2 years. As such:
The suicide death median age is significantly higher for overseas born Australia.
For longer settled migrant communities, the much higher median age suggests that attention be paid to the life experience of older migrants and that potentially growing older in Australia can be associated with higher levels of suicide death and suicidality.
The implication is to consider suicide prevention for this older post war overseas born cohort. The second is by individual countries of birth.
Rate of suicide x country of birth
The ABS Report identifies and enumerates rates of suicide by country of birth.
The graph below shows age-standardised suicide rates by country of birth for those who died by suicide in Australia in 2020-2024. This graph is presented by the highest age-standardised death rate.
Age-standardised suicide rates by country of birth, 2020-2024
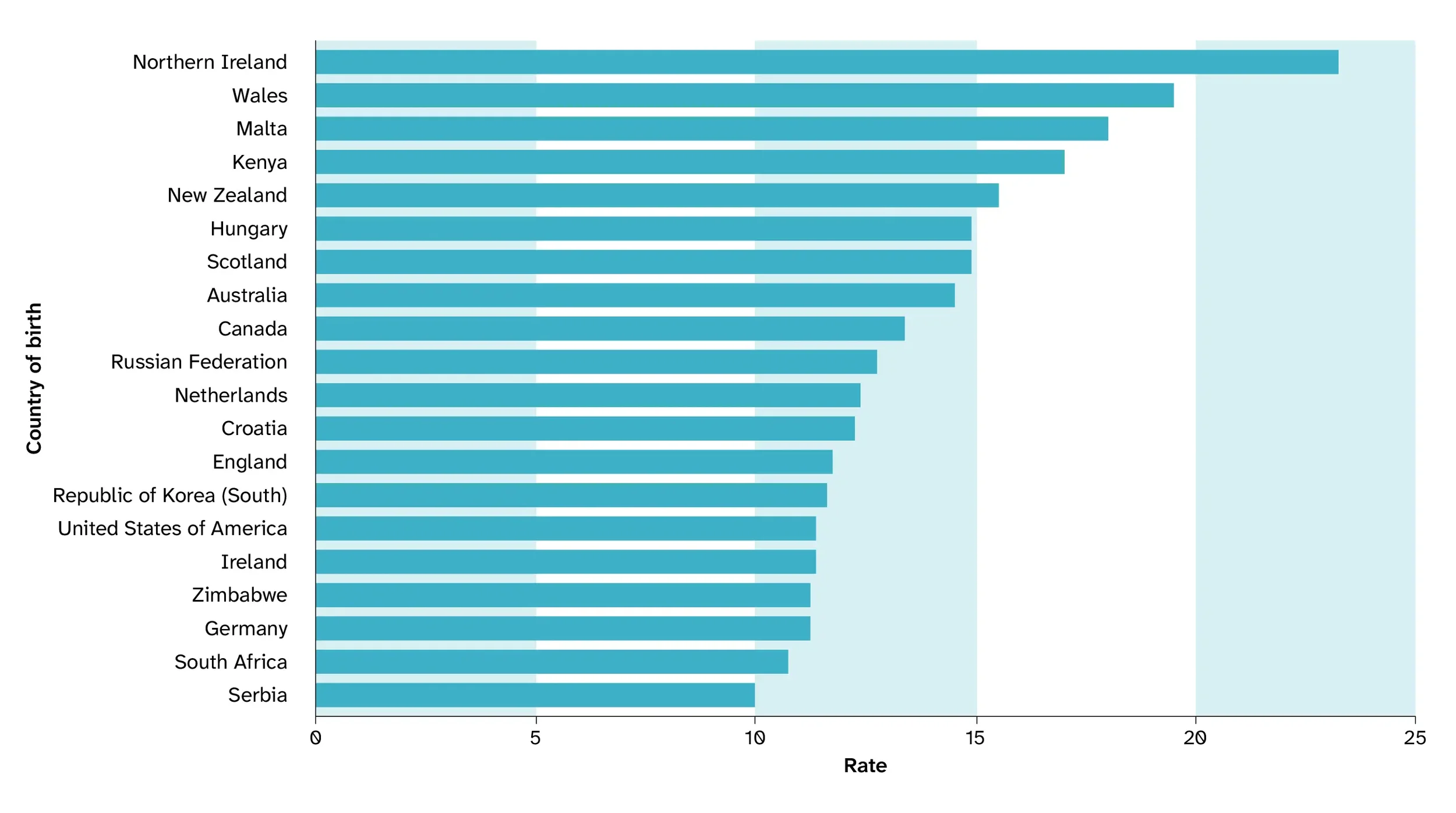
Above: This bar chart shows the suicide rates by the top 20 countries of birth in Australia between 2020 and 2024. The countries listed from highest to lowest are Northern Ireland, Wales, Malta, Kenya, New Zealand, Hungary, Scotland, Australia, Canada, Russian Federation, Netherlands, Croatia, England, Republic of Korea (South), USA, Ireland, Zimbabwe, Germany, South Africa and Serbia.
For the five-year period from 2020 to 2024, the highest rate of suicide for those born in mainly non-English-speaking countries were recorded for those born in Malta, Kenya and Hungary.
Malta and Hungry represent two COB groups with a long migration history and who have a significant older age profile. The ABS 2021 Census indicated that in these communities the percentage aged over 65 were 77% for Malta (27,140 people) and 57% for Hungary (16,655 people).
The rate of suicide for Kenyan-born residents is difficult to interpret but interesting nonetheless, as it is a more recently arrived community which is counter intuitive given the previous point and is predominantly made up of higher educated and English-speaking migrants, arriving under mainly skills and student visas.
Inevitably, the data raises more questions than it answers. It does not provide a firm base to understand suicide in CALD communities and it certainly does not provide the level of granular detail needed to inform policy or strategy settings, or to direct targeted suicide prevention research and initiatives.
Conclusion
Having good data around suicide that captures all demographic segments in Australia is essential. The situation we now have does not allow any meaningful analysis and, as a consequence, cannot adequately inform suicide prevention considerations or approaches.
Our agenda for change must include:
Determining a minimum ethnicity data set for all matters relating to suicide.
Ensuring comprehensive data capture across agencies and jurisdictions including, funerial, coronial and police reporting.
Developing defacto measures and considerations to focus initial attention to suicide in CALD communities that may include aging, have trauma related migration and experience other societal factors such as poverty.
Support is available
The following organisations provide confidential support, guidance and resources to help in navigating challenging times.
Beyond Blue
1300 224 636
Lifeline
13 11 14
Transcultural Mental Health
1800 648 911
Embrace Multicultural Mental Health Services
embracementalhealth.org.au
13YARN
13 92 76
Follow us on LinkedIn to keep informed on communication and engagement matters important to Australia’s CALD communities.